Clinical Studies of the Division of Trauma Surgery
Transcriptomic profiling in severely injured patients
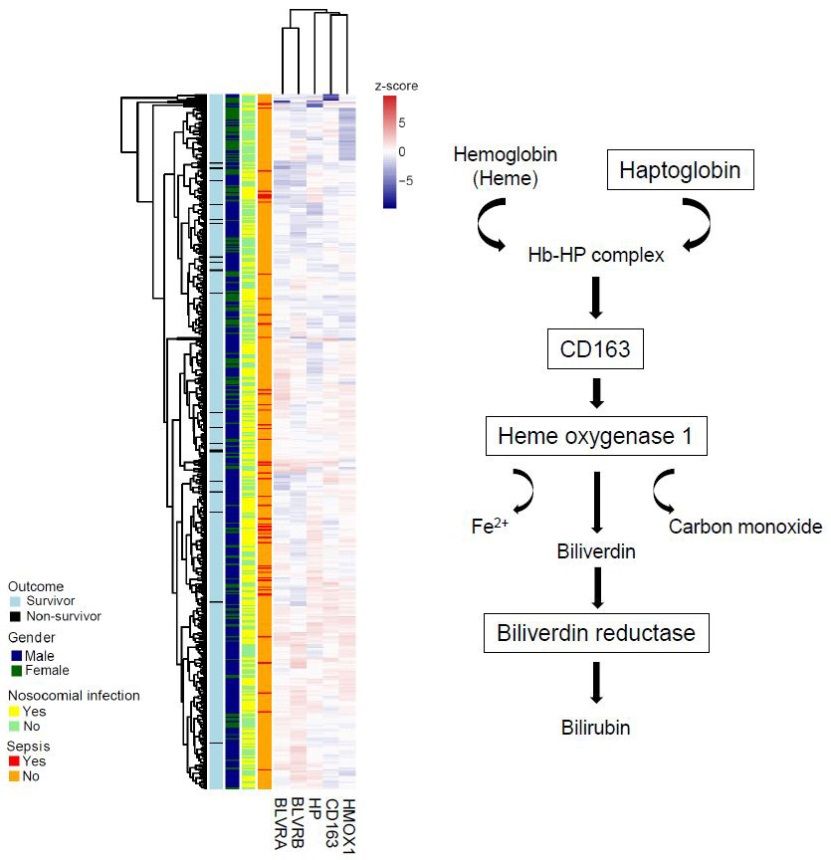
In severe trauma, overwhelming systemic inflammation can result in adverse events and the development of complications, including sepsis. Our studies aim at the identification of mechanisms linked to complicated courses after severe trauma by a systems biology approach. We perform prospective studies by using RNA samples from circulating leukocytes from patients with multiple injuries and analyze the dynamic changes in gene expression over a period of 21 days. Transcriptome profiling is then combined with an extensive clinical data analysis in order to identify prognostic markers characteristic for systemic inflammation and sepsis. The data obtained is of great importance for defining the appropriate treatment of the patients.
SCIentinel study – prospective multicenter study to define the spinal cord injury-induced immune depression syndrome (SCI-IDS)
Infections are the leading cause of death in the acute phase following spinal cord injury and qualify as independent risk factor for poor neurological outcome („disease modifying factor“). The enhanced susceptibility for infections is not stringently explained by the increased risk of aspiration in tetraplegic patients, neurogenic bladder dysfunction, or by high-dose methylprednisolone treatment. Experimental and clinical pilot data suggest that spinal cord injury disrupts the balanced interplay between the central nervous system and the immune system. The primary hypothesis is that the Spinal Cord Injury-induced Immune Depression Syndrome (SCI-IDS) is ’neurogenic‘ including deactivation of adaptive and innate immunity with decreased HLA-DR expression on monocytes as a key surrogate parameter. Secondary hypotheses are that the Immune Depression Syndrome is i) injury level- and ii) severity-dependent, iii) triggers transient lymphopenia, and iv) causes qualitative functional leukocyte deficits, which may endure the post-acute phase after spinal cord injury. SCIentinel is a prospective, international, multicenter study aiming to recruit patients with acute spinal cord injury or control patients with acute vertebral fracture without neurological deficits scheduled for spinal surgery. The objectives are to characterize the dysfunction of the innate and adaptive immune system after spinal cord injury and to explore its proposed ’neurogenic‘ origin by analyzing its correlation with lesion height and severity. This study is a multicentric collaboration between the University Hospital Zurich, the Balgrist Hospital in Zurich, the Charité and the Trauma Hospital in Berlin and the University Hospital in Toronto. More information on the project can be found in Kopp et al. BMC Neurology 2013, 13:168.
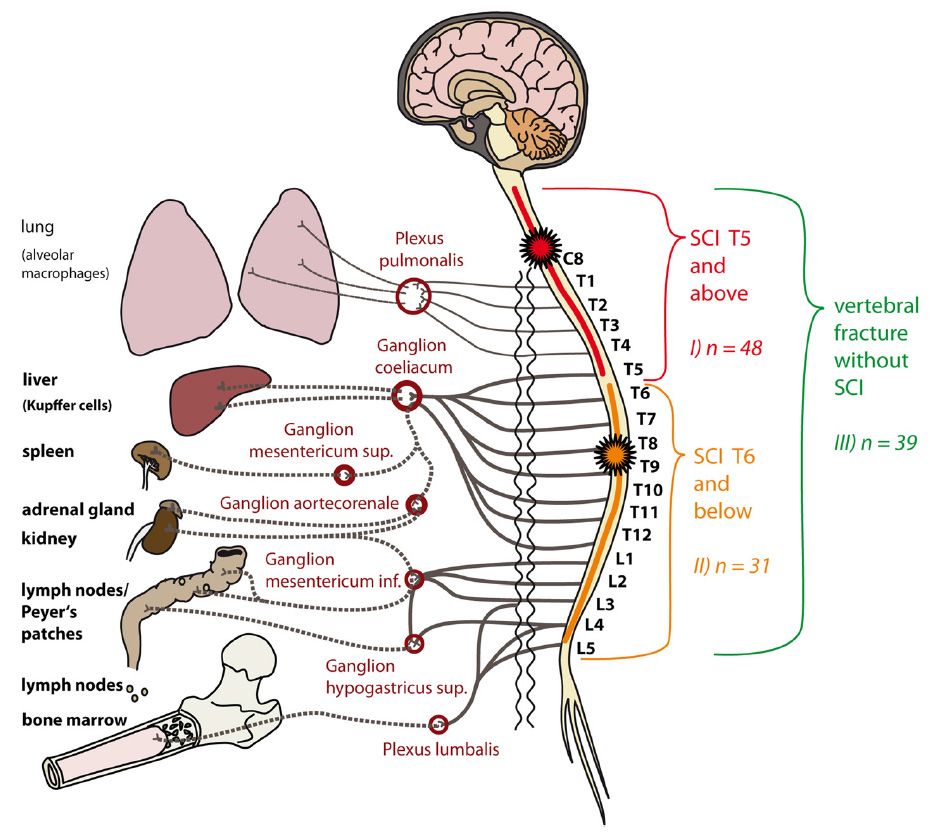
Figure: Relay-interaction of the immune system and the central nervous system. Groups for primary comparison in relation to the major sympathetic outflow (vegetative innervation). In Group I (SCI of the neurological level T4 or above) the lesion is localized within the spinal segments C2-T5, resulting in a disturbance of the sympathetic innervation of immunologically relevant organs through the coeliac ganglion and further ganglia connected through lower segments of the spinal cord. Of note, the neurological level is defined by the ISNCSCI as the most cranial segment with normal sensory function and a muscle grade of at least 3/5 with normal function in the segments above on both sides of the body, i.e. in case of a neurological level T4, the lesion begins in the segment T5. In Group II (SCI of the neurological level T5 or below) the lesion is located in the spinal segment T6 or below. Thus, the sympathetic outflow to the coeliac ganglion is expected being only partially disrupted or completely preserved. Group III consists of patients with vertebral fracture alone without injury to the spinal cord (control). Here, the sympathetic innervation is intact.From Kopp et al. BMC Neurology2013, 13:168.